WHO Standardised Definitions
The WHO CRES technical working group reviewed the WHO standardised definitions and adopted minor clarifications to resolve areas of common misunderstanding. The clarifications are not revisions and the definitions maintain a consistent standard that allows for comparison between studies. Three issues were addressed:
- Consolidation size
The definitions require that consolidation occupy a ‘whole or portion of a lobe’, however there was no specification for what might define the size of a portion. It is possible that different interpretations of this definition led to variation in the identification of consolidation between studies. A footnote clarifying this size is intended to ensure that very small areas of consolidation, even if homogenous, do not constitute endpoint consolidation and help to better distinguish between endpoint consolidation and other infiltrates. - Silhouette sign
A previous footnote explaining the silhouette sign provided a restrictive definition limited to the mediastinal border and also lacked a reference to size. To clarify the value of the silhouette sign in identifying cases of endpoint consolidation, a footnote now specifies that the loss of an anatomic border with the heart or diaphragm should reference the same size definition used for endpoint consolidation.
- Other terminology
The term “dense or fluffy” was an ambiguous descriptor of consolidation and has been replaced by “dense and/or confluent” to explain that while an opacity may completely obscure other anatomical features (i.e. be “dense”), it may also be represented by a single area of opaqueness with varying degrees of opacification (i.e. “confluent”). Similarly, a notation that other infiltrates needed to involve both lungs was removed as this definition was never intended to refer to bilateral findings only.
Definitions
The table below outlines the definitions used for the standardised interpretation of chest radiographs for the diagnosis of childhood pneumonia in epidemiological studies. Conclusion and quality assessment are derived from an interpretation of the findings present on each radiograph. Note that knowledge of the written definitions alone is not sufficient for effective and consistent use of the WHO Radiological Pneumonia standard. Training in the use of the definitions with the reference images to which they have been validated is also essential.
| Finding | Definition | Example | |
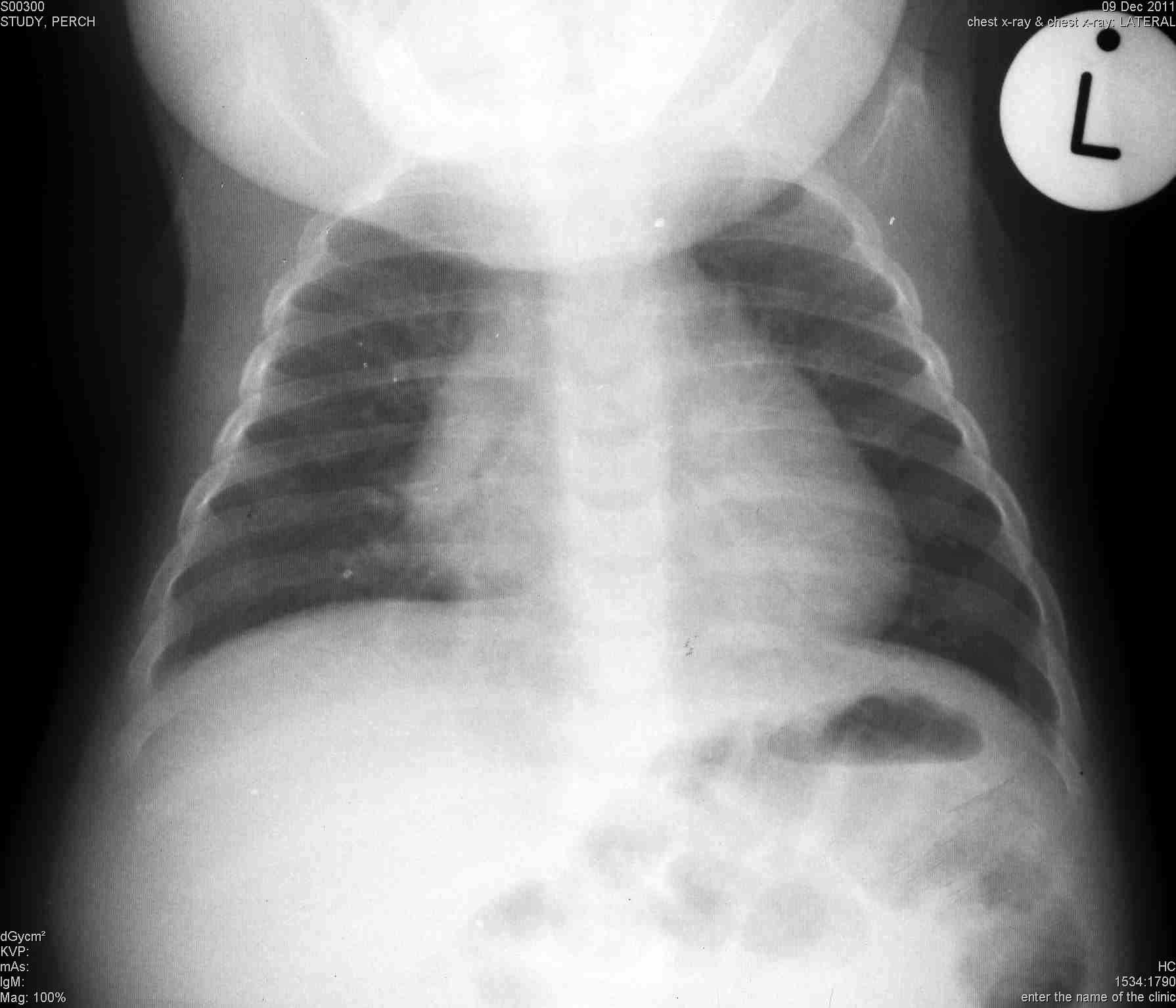
| Quality | Uninterpretable | Features of the image are not interpretable with respect to presence or absence of consolidation or pleural effusion without additional images | |
| Suboptimal | Features allow interpretation of consolidation and pleural effusion, but not of other infiltrates or findings. | ||
| Adequate | Features allow confident interpretation of consolidation and pleural effusion as well as other infiltrates | ||
| Classification of findings | Significant pathology | Refers specifically to the presence of consolidation, infiltrates, or effusion | |
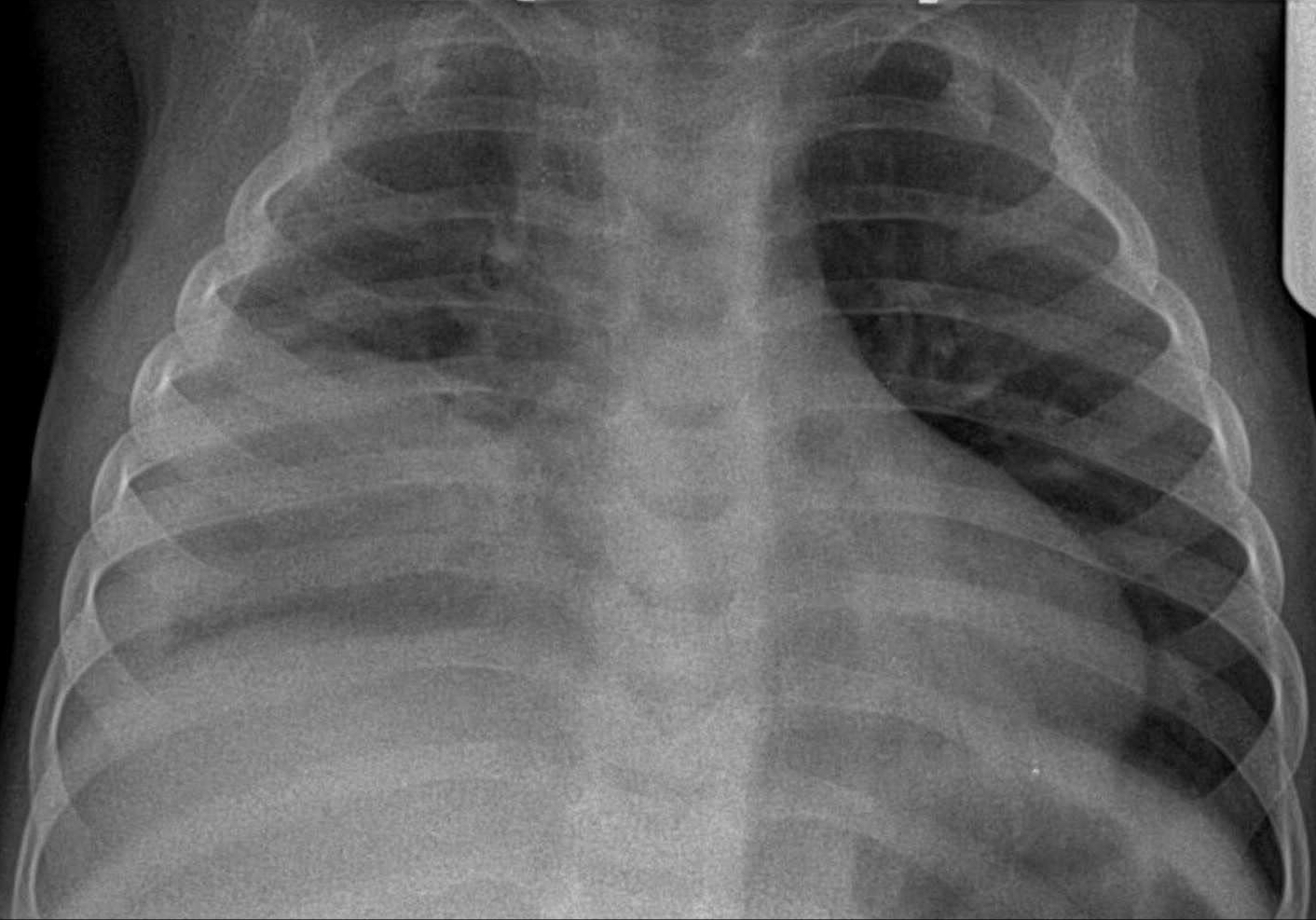
| End-point consolidation a | A dense and/or confluent opacity that occupies a portionb or whole of a lobe or of the entire lung; the presence of air bronchograms indicates consolidation, whereas a silhouette sign indicates the loss of a normally visible border due to the presence of consolidation adjacent to itc | ||
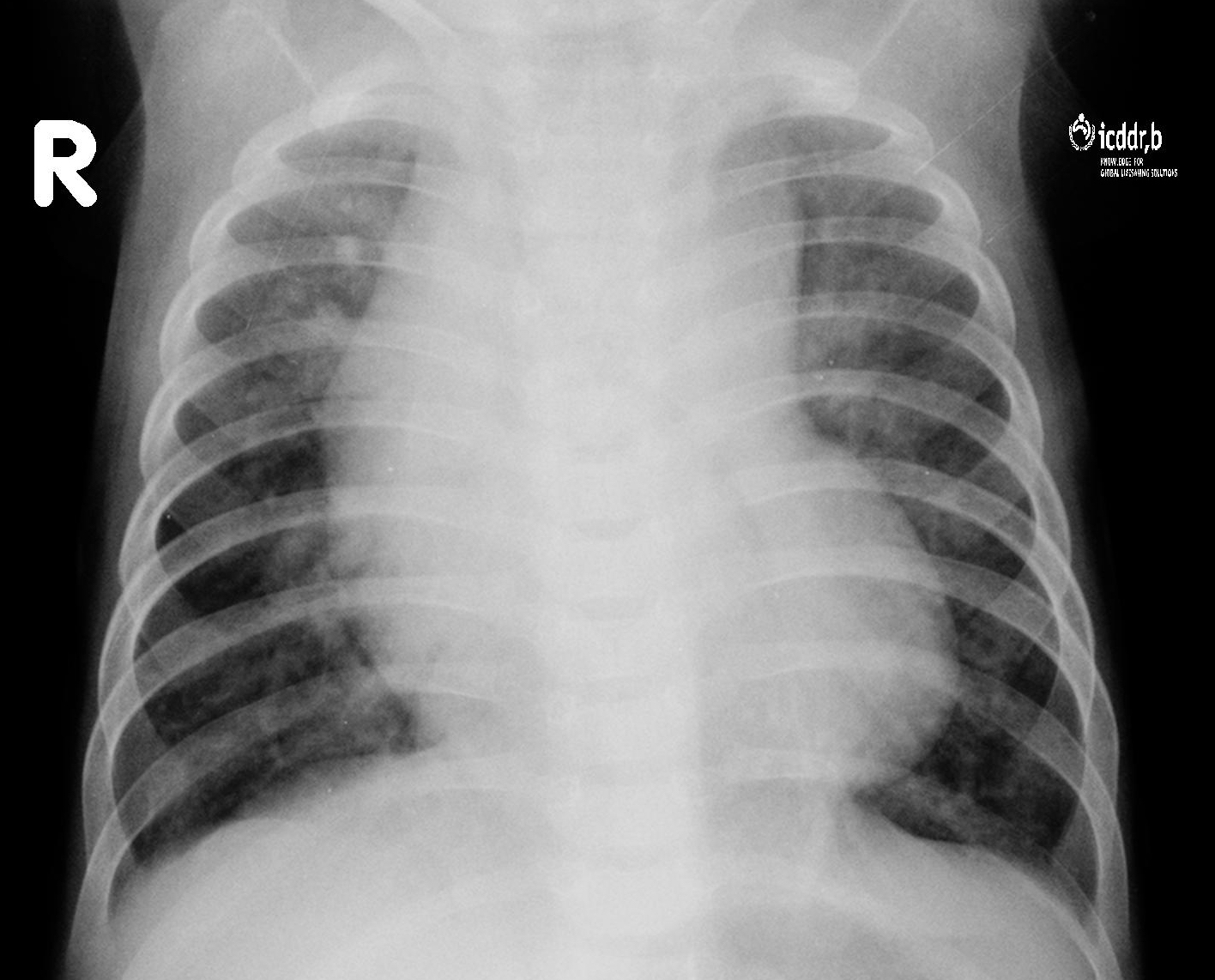
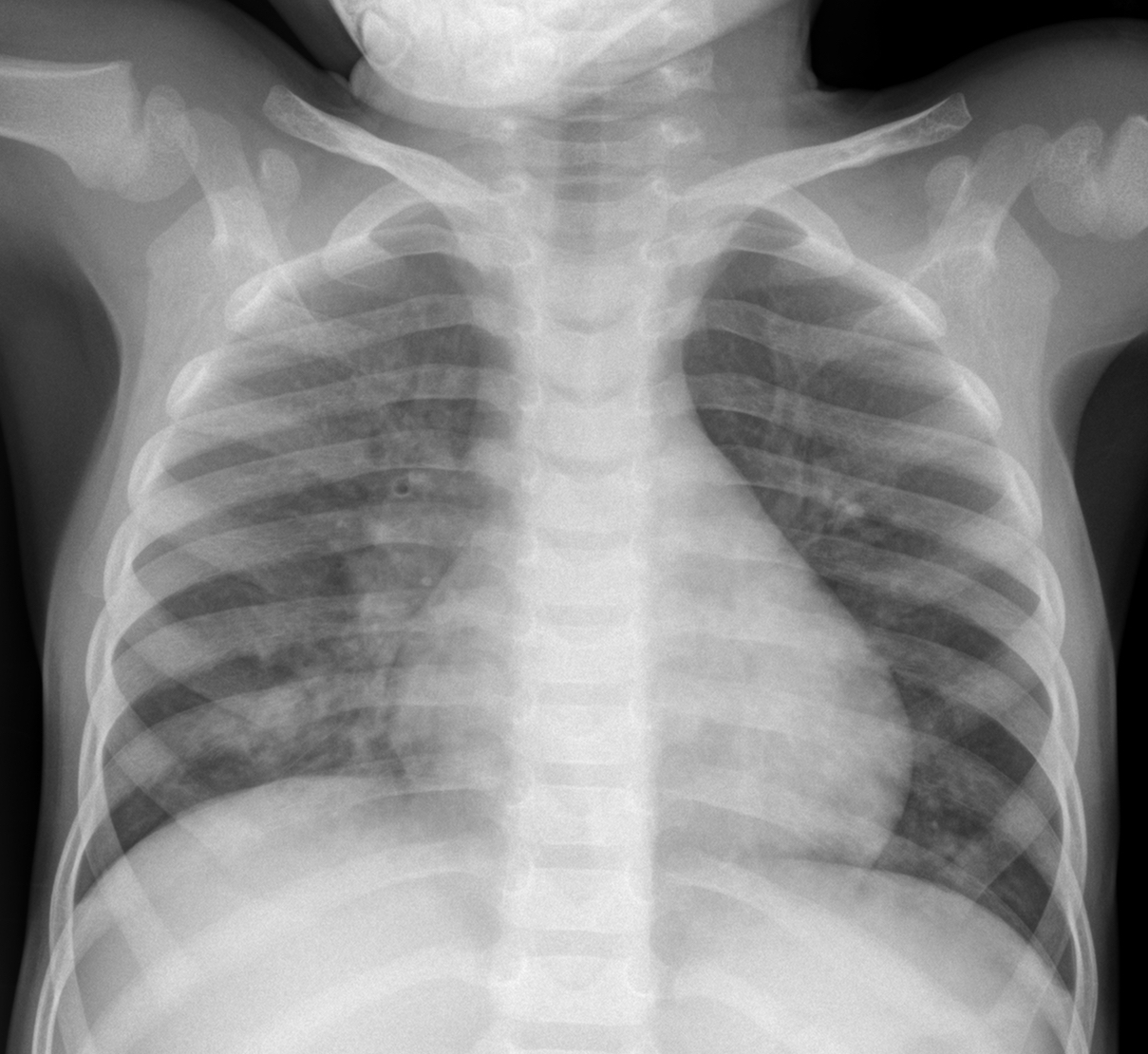
| Other (non-end-point) infiltrates | Linear and patchy opacities (interstitial infiltrate) in a lacy pattern, featuring peribronchial thickening and multiple areas of atelectasis; it also includes minor patchy infiltrates that are not of sufficient magnitude to constitute end-point consolidation, and small areas of atelectasis which in children may be difficult to distinguish from consolidation | ||
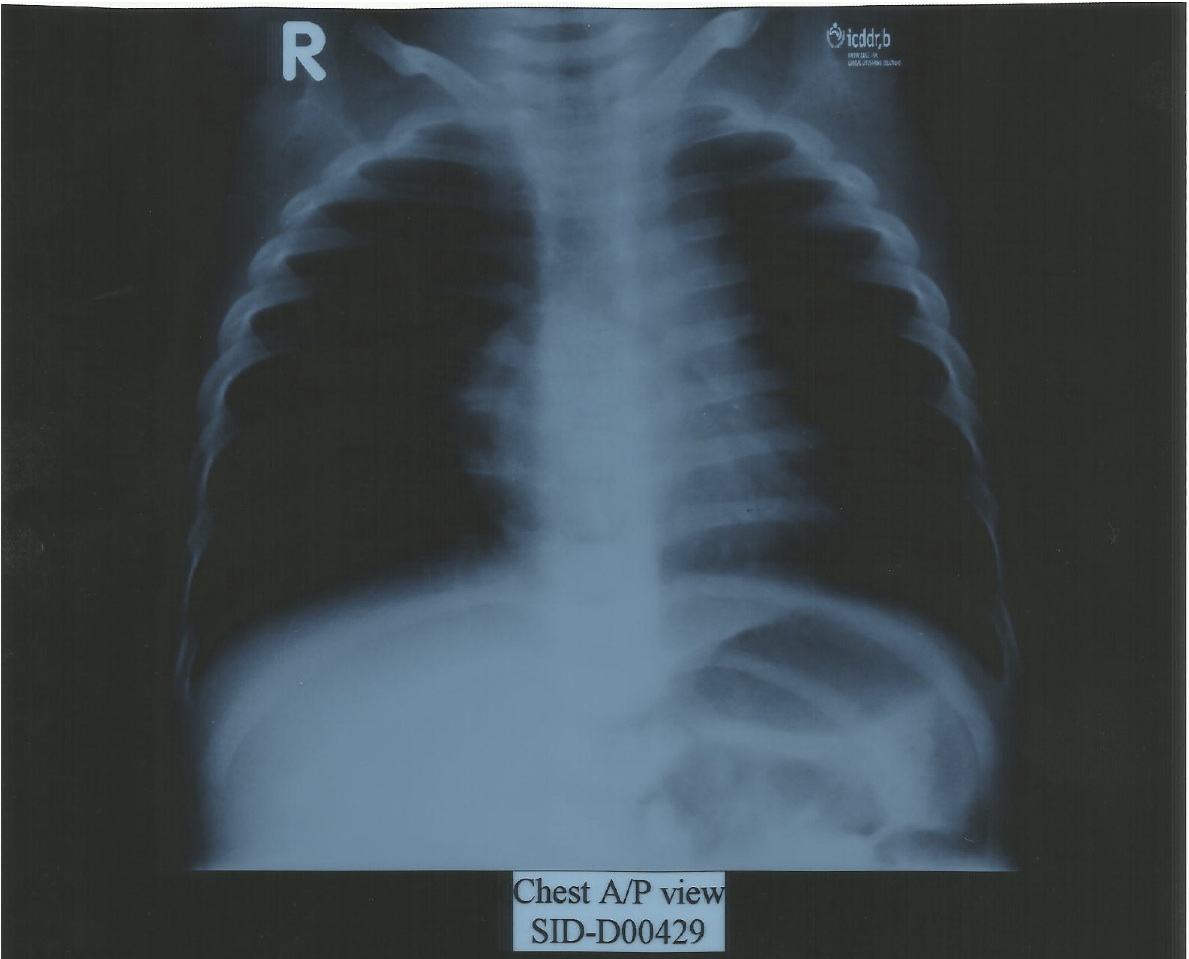
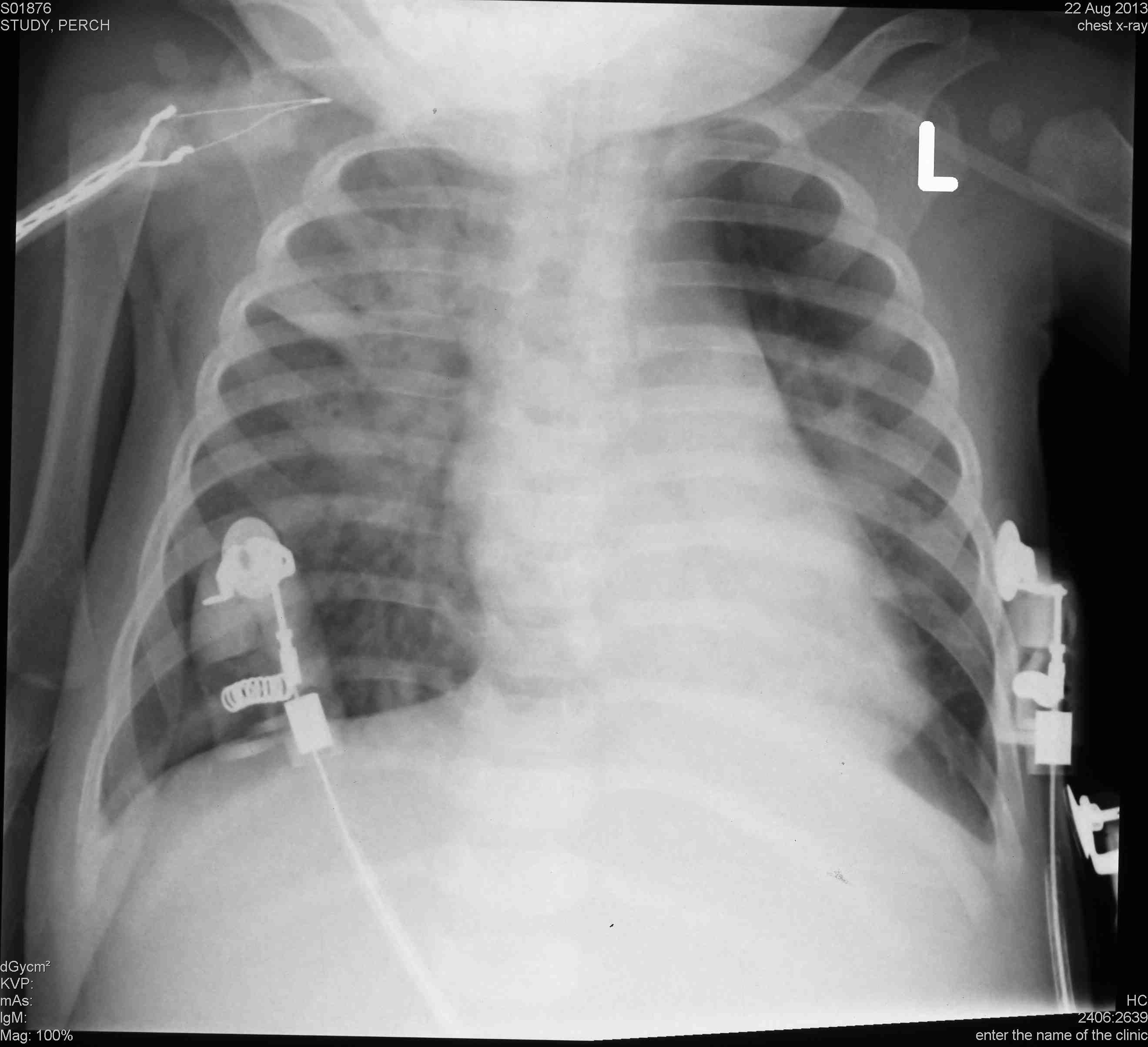
| Pleural effusion | Presence of fluid in the lateral pleural space between the lung and chest wall that is spatially associated with a pulmonary parenchymal infiltrate (including other infiltrate) or has obliterated enough of the hemithorax to obscure any infiltrate; in most cases, this will be seen at the costo-phrenic angle or as a layer of fluid adjacent to the lateral chest wall; this does not include fluid seen in the horizontal or oblique fissures | ||
| Conclusions d | Primary end-point pneumonia | The presence of consolidation or pleural effusion, as defined above | |
| Other infiltrate | The presence of other (non-consolidation) infiltrate as defined above in the absence of a pleural effusion | ||
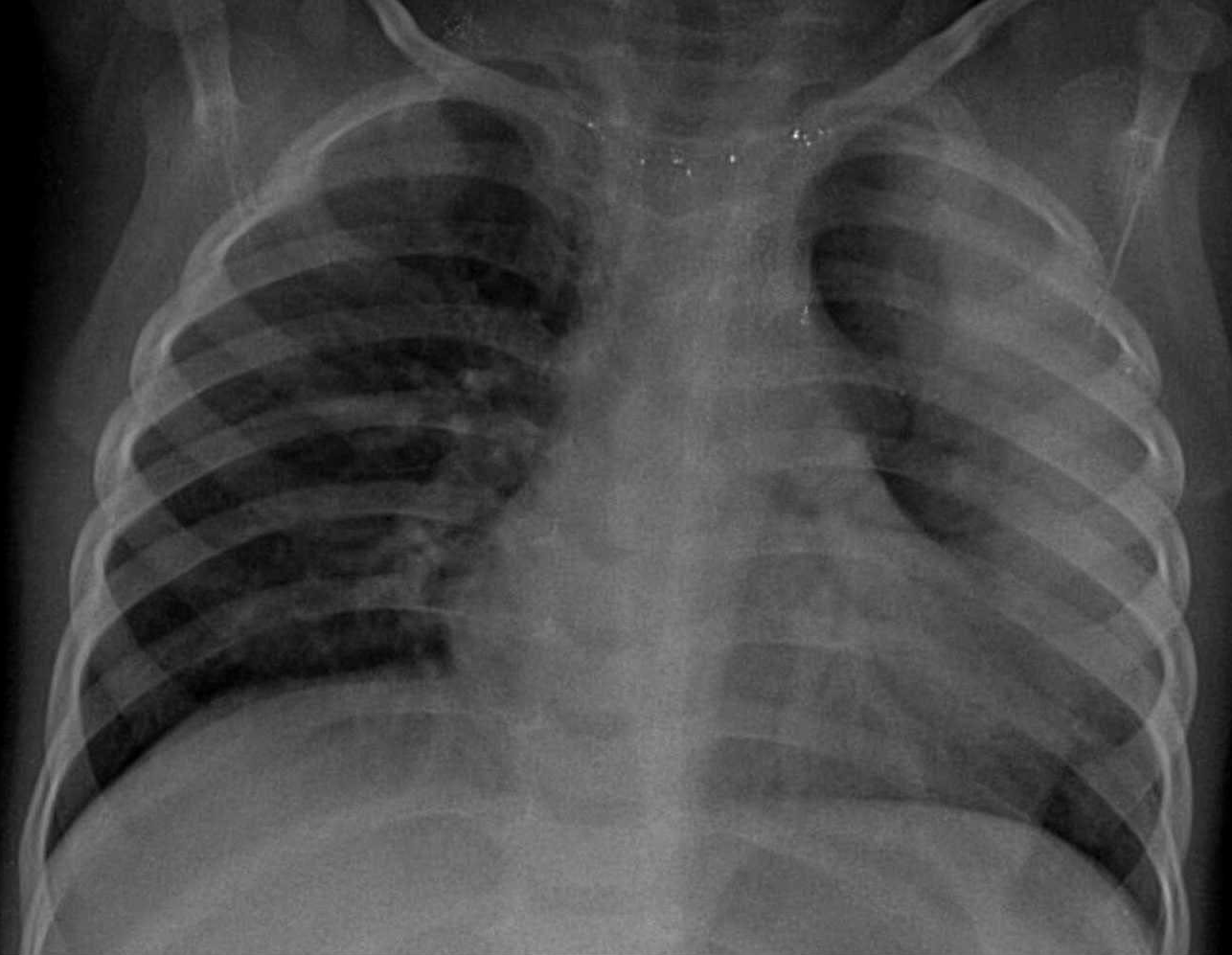
| No consolidation / infiltrate / effusion | Absence of consolidation, other infiltrate, or pleural effusion |
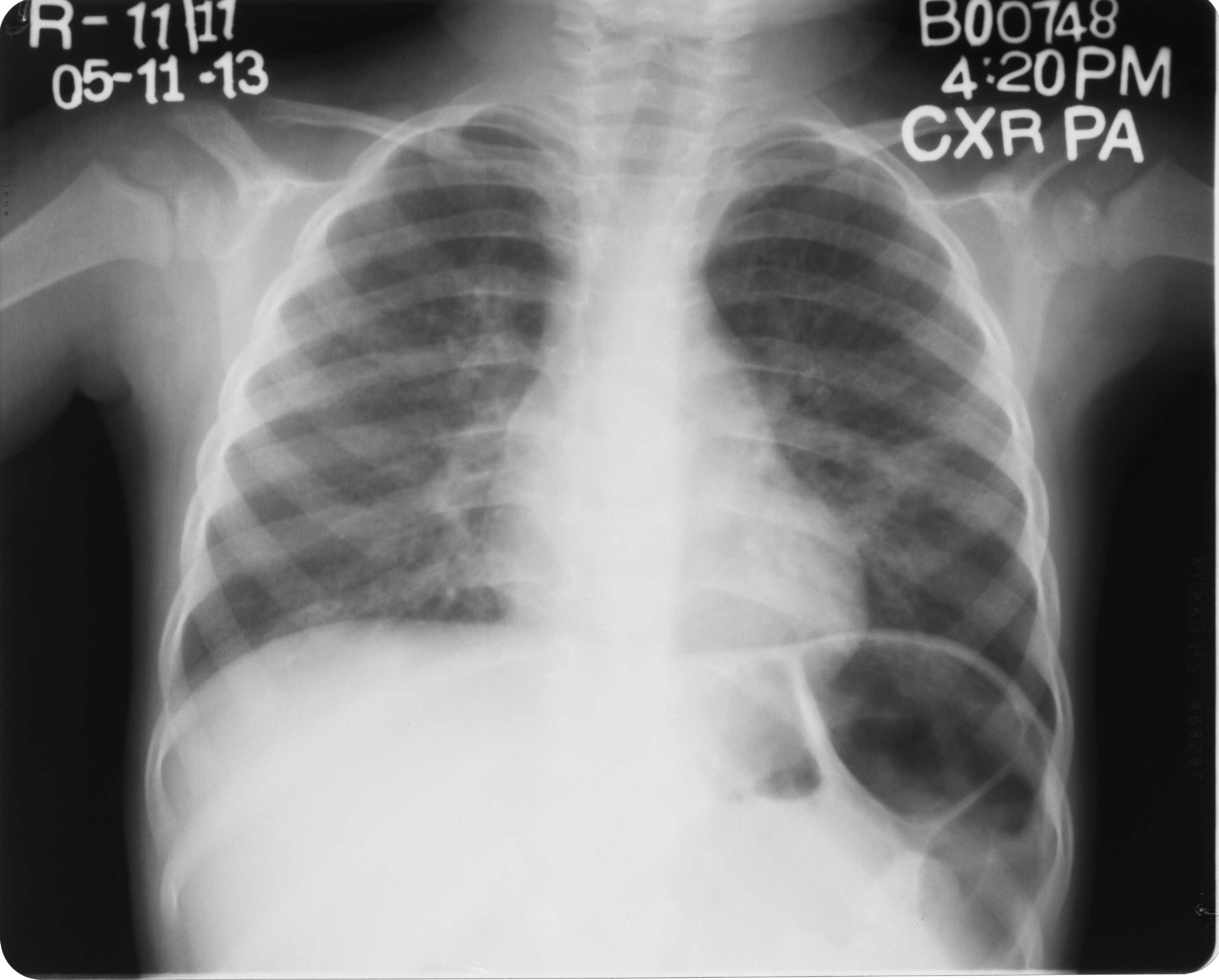

a Term “end-point” refers to this being the end-point of interest for trials of bacterial vaccines against pneumonia.
b “Portion of a lobe” means opacity with the smallest diameter greater or equal to the size of a posterior rib and one adjacent rib space at the same level as the opacity. Where the opacity is irregular in shape (e.g. wedge-shaped), use the maximum short-axis diameter (the largest diameter perpendicular to the line of maximum diameter of the opacity)
c In the presence of any visible adjacent opacity, a silhouette sign is indicative of consolidation if the size of loss of the anatomical border is greater or equal to the total size of a posterior rib together with one adjacent rib space at the same level. A silhouette sign of this size without a visible adjacent opacity is considered other infiltrate.
d Refers to the presence of these conclusions in the opinion of a panel of trained readers using the available World Health Organization defined reference materials and methods.